
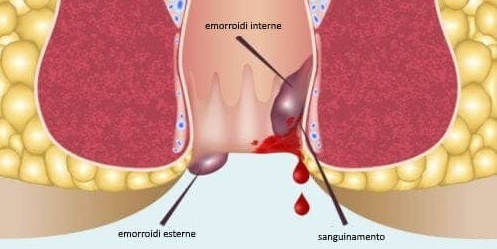
The “hemorrhoids” are venous structures located in the last part of the digestive tract and physiologically contribute to the drainage of the rectal ampulla and the last part of the anal canal. Hemorrhoidal disease is a common condition in countries with a high standard of living and it is estimated that in Western countries half of the population over the age of 35 is affected more or less severely by this disease with a slight prevalence for women.
Favorable factors are prolonged standing, sedentary lifestyle, obesity, such as a low-slag diet and constipation.
The “hemorrhoids” are venous structures located in the last part of the digestive tract and physiologically contribute to the drainage of the rectal ampulla and the last part of the anal canal. Despite the development over the years of numerous techniques (demolition or conservative surgery, elastic ligation, laser, cryotherapy), attention is currently being focused on the search for an ideal method: that is, painless, outpatient, repeatable and possibly without complications.
These criteria correspond to sclerosis with mousse with a flexible endoscope.
The pathophysiological assumption of the sclerosing foam method is to create an inflammatory reaction (a principle transferred from experience in the phlebological field for the treatment of varices of the lower limbs) and to induce a vessel spasm with progressive “sclerosis” of the haemorrhoidal prolapse and bleeding.
The procedure is performed without anesthesia by using a flexible endoscope in the absence of pain during the injection as it pricks an area without sensory innervation. A direct method was recently developed at the Hippocrates Center, ie without the need to resort to the endoscope, but to be performed with a simple anoscope and with direct puncture of the affected vessel with particular thin needles of appropriate length and flexibility. The experience over many years of venous sclerotherapy transferred to proctology has made it possible to lower the concentrations of sclerosing drug optimizing the results, practically eliminating complications, at the cost of repeating the procedure and fortnightly checks in the first 2 months.
At the end of the procedure, the patient can resume all his activities and the method is outpatient.
The complete absence of pain during and only a slight discomfort in the days following the procedure and the absence of hospitalization were particularly appreciated by patients.
The method is particularly effective in cases of haemorrhoidal bleeding with satisfactory results in all patients treated.
With haemorrhoidal endosclerosis with foam, we can say that the traditional surgical procedure should be reserved only for really complicated cases associated with other pathologies of the anorectal sphere such as prolapse and neoplasms.